The Allelica Multi-Ancestry CAD PRS report: what clinicians receive and how to use it

Preventive cardiology focuses on reducing lifetime atherosclerotic cardiovascular disease risk by intervening early and proportionately. Traditional tools, including pooled cohort equations, lipid measurements, and coronary calcium scoring, primarily estimate near term risk and may underestimate lifelong susceptibility in certain patients.
The Allelica Multi-Ancestry CAD Polygenic Risk Score Report provides a structured assessment of inherited CAD risk that complements existing risk stratification tools. It is designed to support clinical decision making in primary prevention, particularly when conventional risk assessment yields uncertainty.
Ancestry-calibrated risk assessment
Each report includes genome-wide ancestry analysis derived from the patient’s genetic information. This analysis is used to ensure appropriate calibration of the polygenic risk score to the relevant reference population for the tested individual.
Because polygenic risk scores are population-dependent, this step is essential for maintaining clinical validity across diverse and admixed patients. As a result, reported percentiles and hazard ratios reflect biological risk rather than demographic approximation.
Core results and interpretation
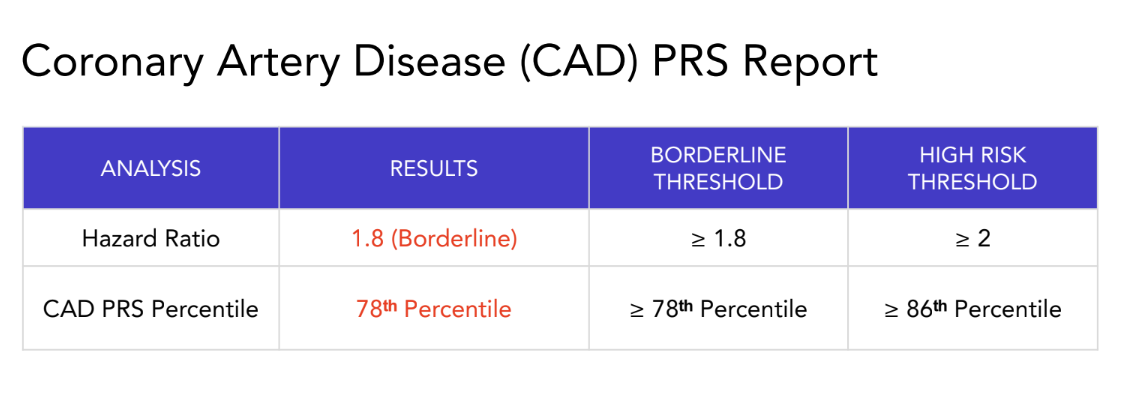
The core of the report is a single results table that summarizes inherited coronary artery disease risk using two standardized measures.
The CAD PRS percentile indicates where the patient falls within the population distribution of genetic risk. A higher percentile reflects greater inherited susceptibility relative to peers of similar ancestry.
The hazard ratio estimates the patient’s risk of coronary artery disease compared with those without high risk. A hazard ratio of 1 represents average risk. Values above 1 indicate proportionally higher lifelong risk and reflect cumulative exposure rather than short-term event probability.
The table also displays predefined risk thresholds that classify results as not elevated, risk-enhancing, or FH equivalent risk. These thresholds appear directly in the table and are aligned with outcome-based evidence and preventive cardiology guidelines.
This format allows clinicians to rapidly assess both the magnitude of inherited risk and its clinical category without additional calculations or genetic interpretation.
Risk-enhancing genetic risk and FH-equivalent risk
Individuals with a polygenic risk score in approximately the top 20 percent of the population have at least a two-fold increased lifetime risk of coronary artery disease. This level of inherited risk functions as an ACC and AHA risk-enhancing factor.
In patients with borderline or intermediate 10-year ASCVD risk by pooled cohort equations, this finding supports shared decision-making and may appropriately tilt management toward statin initiation or intensification. In this setting, polygenic risk refines risk assessment when traditional tools alone do not provide clear direction.
When the polygenic risk score falls within approximately the top 10 percent of the population, depending on the ancestry, the report identifies very high genetic risk. This level of risk corresponds to a three-fold or greater increase in lifetime CAD risk and is comparable to monogenic familial hypercholesterolemia.
Patients in this category may have LDL-C levels below traditional familial hypercholesterolemia thresholds, minimal coronary calcium early in life, or low estimated short term risk. Despite this, their inherited susceptibility supports earlier and more intensive preventive management.
The report contextualizes this risk using familiar clinical analogues, supporting treatment approaches similar to those used for familial hypercholesterolemia, including early high-intensity statin therapy and use of nonstatin agents to achieve guideline-recommended LDL-C targets

Summary
The report includes a concise summary that translates the polygenic risk score into clear clinical language describing the magnitude of lifetime CAD risk. This summary is designed for direct incorporation into clinical documentation and care coordination.
Clinical implications section
The Implications section links genetic risk categories to preventive strategies already familiar to cardiologists. This section references earlier or more intensive lipid-lowering therapy, consideration of advanced imaging when clinically appropriate, comprehensive risk factor management, and attention to family risk.
This section does not prescribe therapy but provides context to support clinical judgment within established preventive cardiology frameworks.

Long term clinical use
The Allelica Multi-Ancestry CAD PRS Report represents a one-time assessment of inherited CAD risk. While the polygenic risk score does not change, its relevance evolves as patients age and as additional risk factors emerge.
Once incorporated into the medical record, the report serves as a durable reference that informs preventive intensity, interpretation of future biomarkers and imaging, and family counseling over time.
By presenting inherited CAD risk in a clear and clinically interpretable format, the Allelica Multi-Ancestry CAD PRS Report supports earlier identification of patients whose lifetime risk is underestimated by traditional risk factors. This enables more precise and timely preventive care.
To learn more or review demo reports, contact us at info@allelica.com.